Healthcare systems globally are being asked to do more with less — while demand rises, workforces remain stretched, and the cost of care continues to climb. Cost intelligence is how leading organizations are finally getting ahead of it.
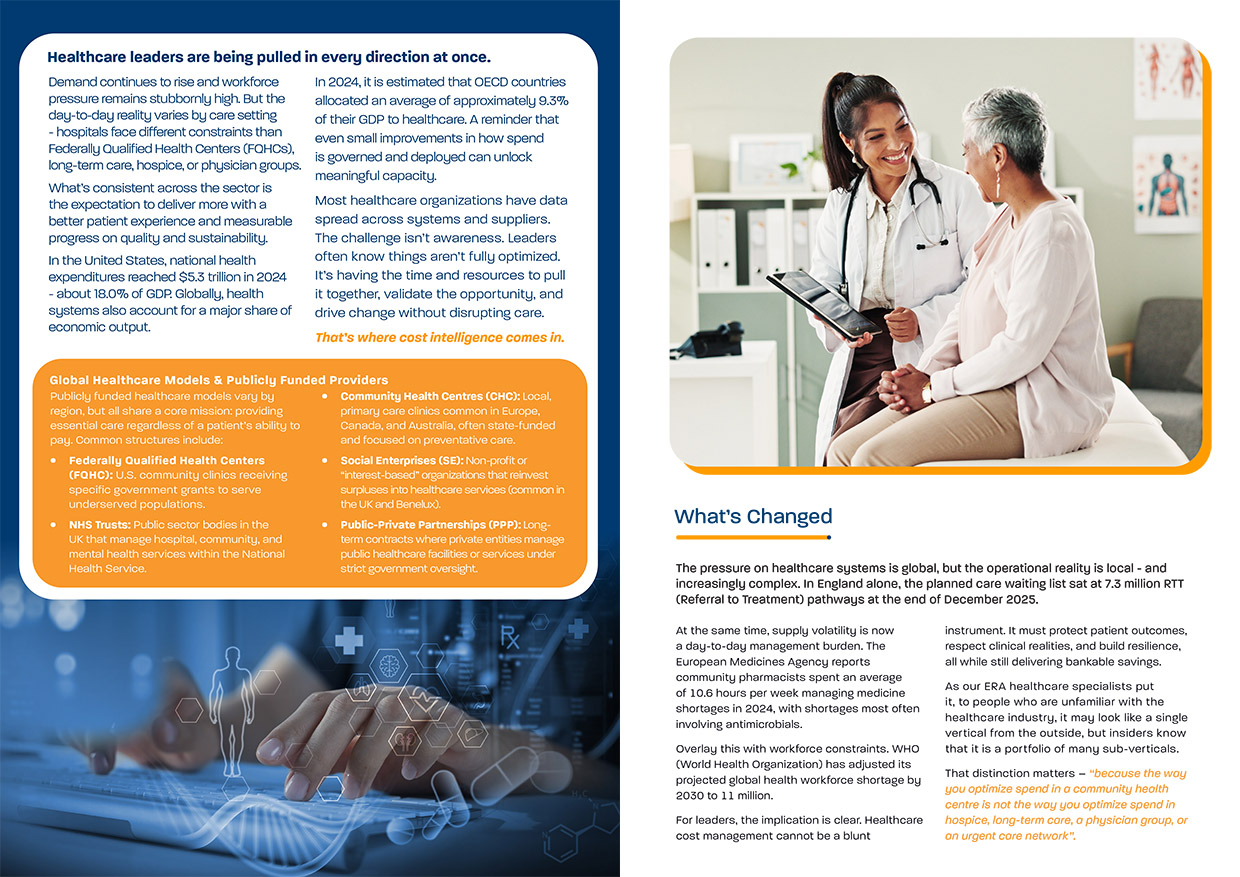
US national health expenditures reached $5.3 trillion in 2024 — approximately 18% of GDP. Across OECD nations, healthcare accounts for roughly 9.3% of economic output. Even small improvements in how spend is governed and deployed can unlock meaningful capacity. Yet most healthcare organizations are sitting on fragmented data: AP files, distributor reports, GPO documentation, and contract folders accumulated over years. Traditional reporting tells you what you spent. It doesn't tell you where the real opportunities are, or how to capture them without disrupting care.That gap is where cost intelligence operates. Unlike blunt cost-cutting, cost intelligence connects spend visibility with category expertise and clinical context — enabling leaders to prioritize, validate, and act on the right opportunities at the right time. ERA Group's healthcare specialists have worked across hospitals, FQHCs, long-term care, hospice, physician groups, and community health networks. Their insight is clear: healthcare looks like one vertical from the outside, but it's a portfolio of sub-verticals — and the way you optimize spend in a community health centre is not the way you optimize it in a hospice, a lab services network, or an urgent care group.This whitepaper explores where cost most commonly hides in healthcare — from clinical consumables and physician preference items to DME rentals and underutilized GPO arrangements — and how ERA's approach surfaces and captures those savings without compromising clinical standards or supplier relationships.

Inside this whitepaper, you'll find: a breakdown of the global healthcare cost landscape and the structural pressures driving it; an honest look at why internal teams struggle to capture savings sustainably; specific examples of where cost hides across clinical and indirect categories; real-world case studies spanning FQHCs, long-term care, hospice, diagnostic providers, and large private groups; and a practical framework for separating what's clinically non-negotiable from what can be safely standardized or renegotiated.ERA's healthcare specialists don't come in to do a slash-and-burn on expenses. The goal is visibility and alignment — protecting what's clinically essential while making everything else more consistent, more transparent, and more affordable.The outcome? Bankable savings that can be reinvested directly into patient care, capacity, and quality improvement — without disrupting the clinical relationships or supplier partnerships that matter most.
The pressure on healthcare systems is global, but the operational reality is local - and increasingly complex. In England alone, the planned care waiting list sat at 7.3 million RTT (Referral to Treatment) pathways at the end of December 2025.
ERA's healthcare specialists don't come in to do a slash-and-burn on expenses. The goal is visibility and alignment — protecting what's clinically essential while making everything else more consistent, more transparent, and more affordable.The outcome? Bankable savings that can be reinvested directly into patient care, capacity, and quality improvement — without disrupting the clinical relationships or supplier partnerships that matter most.
Kaynağı indirin